
SIJ Institute
Focused relief for sacroiliac joint pain.
Browse anatomy, diagnosis, treatments, research, real case examples, and consultation details in one place, with the same core information as the main site arranged for smaller screens.
About SIJ
What is the sacroiliac joint?
The sacroiliac joint connects the sacrum to the iliac bones of the pelvis. It helps transmit load between the spine and legs, supports stability, and absorbs forces during daily movement.
When the SI joint becomes inflamed, unstable, degenerative, or overloaded, it can create pain that overlaps with spine, hip, and pelvic conditions.
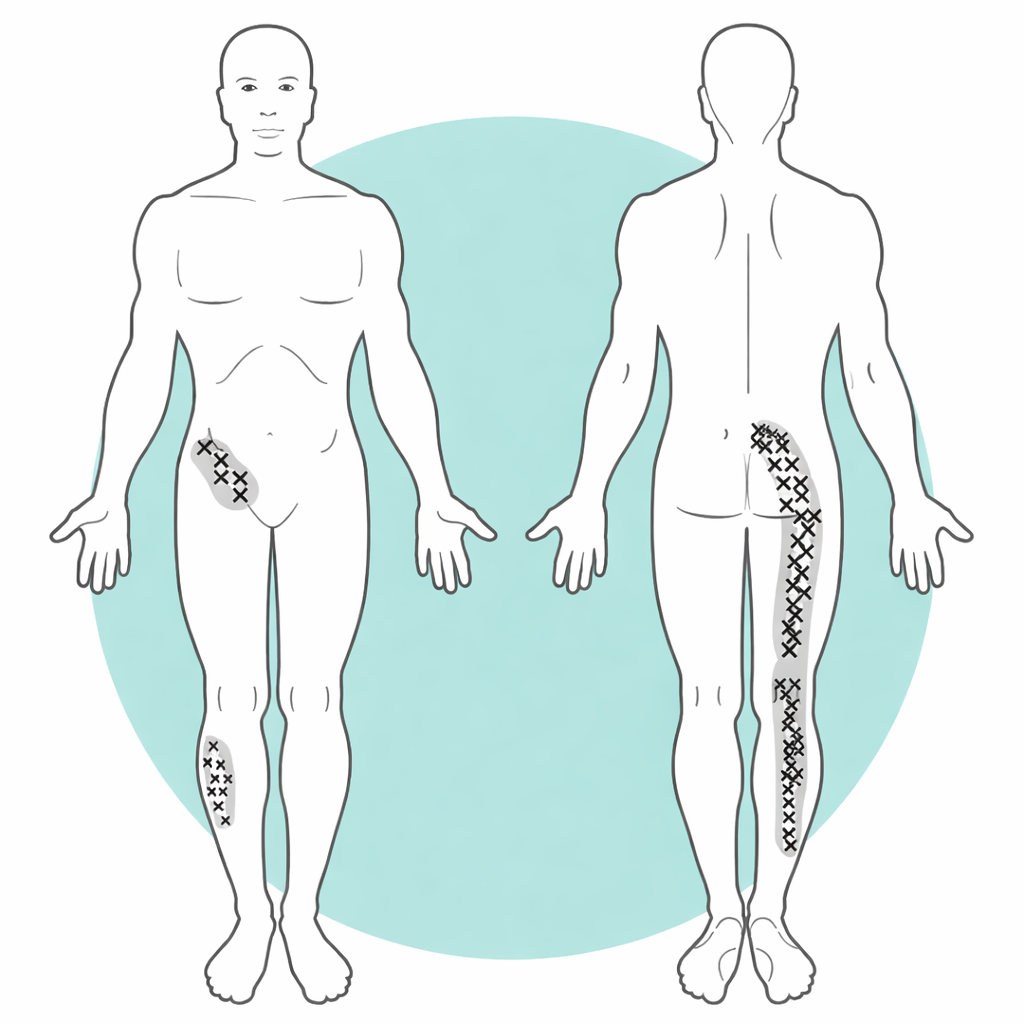
Patients may experience lower back pain, buttock pain, groin discomfort, pelvic pain, and sometimes pain that travels into the thigh or leg.
Because the SI joint sits close to other pain-generating structures, symptoms are often mistaken for lumbar disc, facet, or hip-related problems.
SIJ Institute is built around clearer evaluation, patient education, and a stepwise treatment pathway specific to sacroiliac joint pain.
The joint helps move force from the upper body into the pelvis and legs during standing, walking, lifting, and changing position.
Even though the SI joint moves only slightly, irritation or abnormal mechanics can still trigger major pain.
Understanding the SI joint helps patients make sense of symptoms that may not match a typical disc or hip problem.
Anatomy
Where the sacroiliac joint sits and why it matters.
The sacroiliac joints sit where the sacrum meets the iliac bones. They transfer force from the upper body into the pelvis and legs while helping maintain stability.
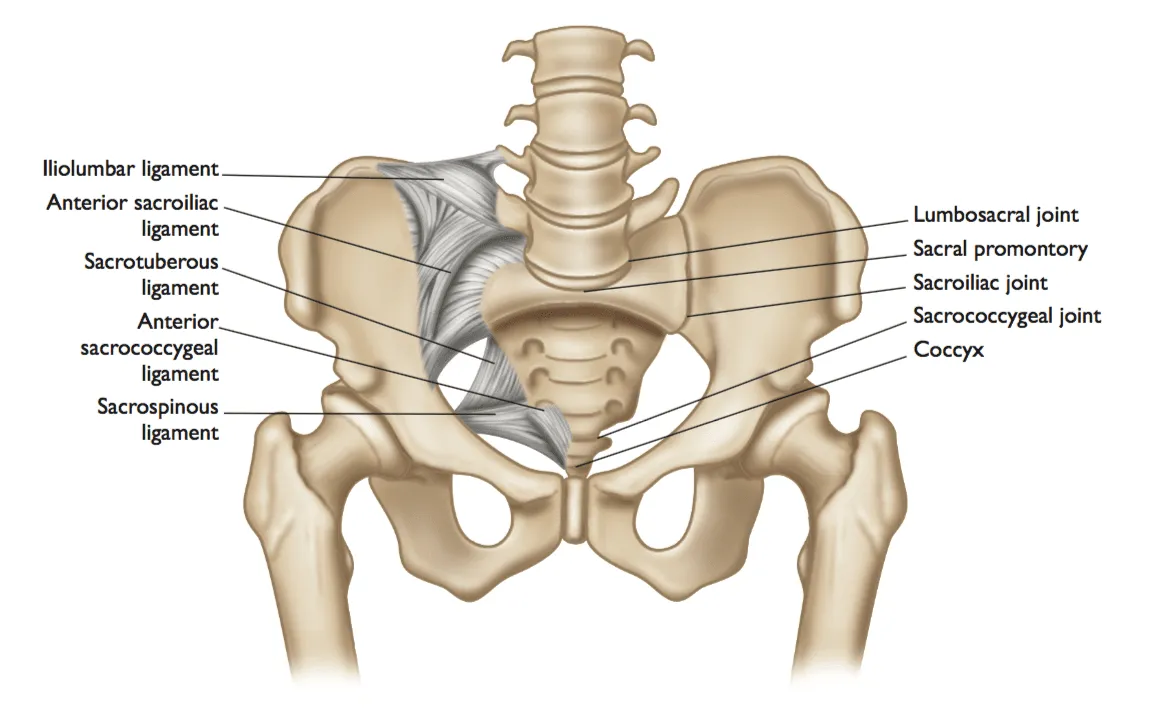
The triangular base of the spine that bridges the lumbar spine and the pelvis.
The broad weight-bearing pelvic surfaces that meet the sacrum at the SI joints.
Much of SI joint stability comes from surrounding ligaments, which can also contribute to pain.
Diagnosis
Separating SI joint pain from other causes.
Diagnosis requires more than a scan alone. SI joint pain is identified through symptom pattern, physical examination, imaging context, and diagnostic testing when needed.
We review where the pain starts, where it travels, how long it has persisted, and what makes it worse.
Provocation maneuvers help determine whether the sacroiliac joint is likely contributing to symptoms.
X-rays, CT, and MRI help clarify anatomy but are always interpreted alongside the broader clinical picture.
Image-guided injections can help confirm the SI joint as the pain generator in selected patients.
Distraction, compression, thigh thrust, FABER, and Gaenslen's testing are commonly used when SI joint pain is suspected.
Disc problems, facet pain, hip disease, piriformis syndrome, and post-surgical back pain can all mimic SI joint dysfunction.
Treatments
A stepwise pathway from conservative care to advanced stabilization.
Movement correction, stabilization, and rehabilitation strategies to improve function and reduce pain.
Selected biologic and regenerative options may be considered within a personalized care plan.
Targeted interventional options for patients needing more durable relief.
For carefully selected patients with persistent SI joint dysfunction, robotic fusion may provide a definitive stabilization option after conservative and minimally invasive treatments have been exhausted.
Structured exercise can produce meaningful long-term improvement, particularly in chronic SI pain before disability becomes more established.
Even after procedures, follow-up, rehabilitation, and activity guidance remain important for durable symptom relief and restored function.
Pain Quiz
Could your symptoms be related to the SI joint?
This short quiz is not a diagnosis, but it can help patients recognize symptom patterns seen in sacroiliac joint dysfunction.
Case Examples
How SIJ cases can look completely different.
A 67-year-old patient from Melbourne had severe back pain after failed physiotherapy, SIJ prolotherapy, and pain management. SIJ injection gave 24 hours of relief, and endoscopic radiofrequency ablation and neurectomy later produced 85% improvement.

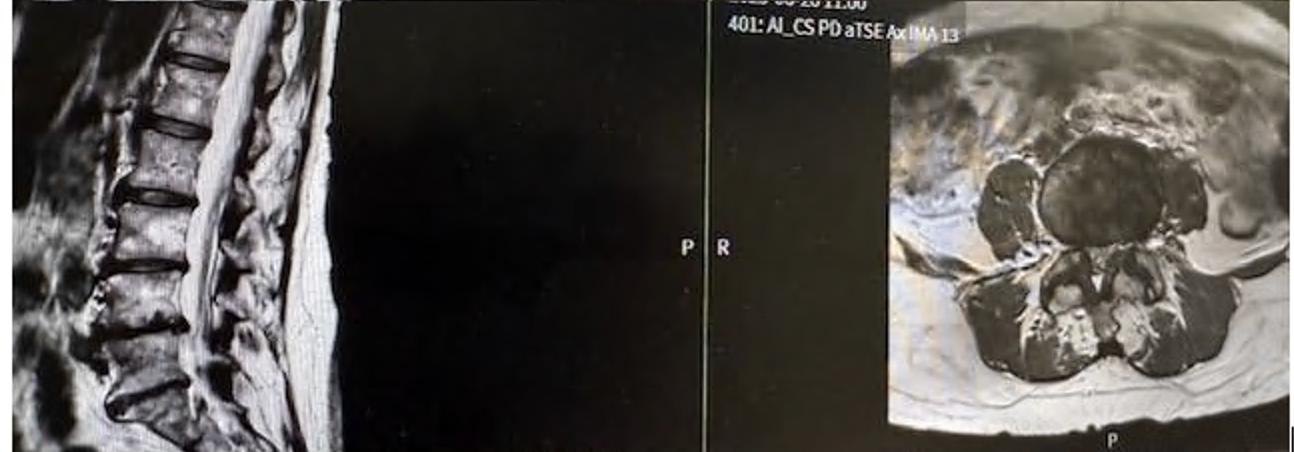
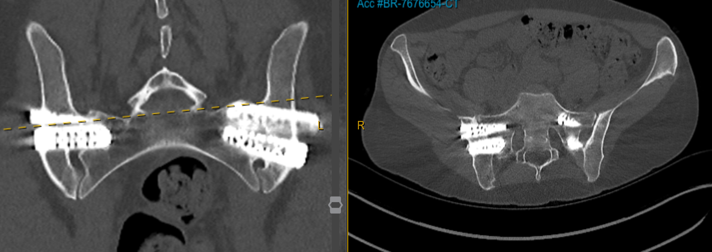
A 75-year-old woman developed right-sided buttock, groin, and leg pain 33 years after an L5/S1 fusion. MRI was limited by artifact, CT showed no major compression, and SIJ injection produced excellent relief.
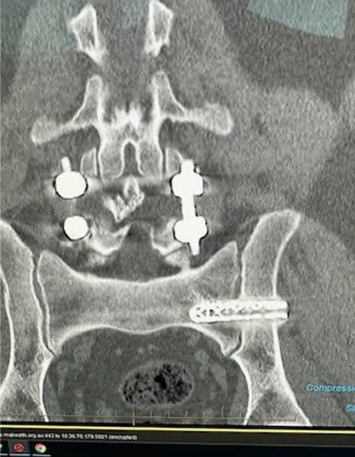
This revision case had already gone through a cluneal nerve stimulator, cluneal nerve radiofrequency ablations, repeat SIJ injection, and repeat SIJ ablation before robotic and endoscopic revision planning was considered.

A 21-year-old active gymnast with hypermobility, several years of back pain, and severe SIJ tenderness underwent multiple prior treatments before robotic sacroiliac joint fusion led to good pain improvement and return to reasonable normal activity.
A 38-year-old psychologist with hypermobile EDS had severe back pain and instability over several years, short-term relief from prolotherapy, and a largely normal lumbar MRI despite major symptoms.
Research
Clinical thinking informed by evolving evidence.
Monitoring literature and clinical outcomes that shape modern SI joint diagnosis and care.
Interest in refining minimally invasive and technology-assisted approaches where appropriate.
Focusing on pain relief, function, mobility, and clearer decision-making across the treatment pathway.
Research helps identify which symptom patterns, imaging findings, and responses to injections most strongly predict meaningful benefit from treatment.
Care Team
Leadership grounded in specialized care and patient trust.
Prashanth Rao is a neurosurgeon with a keen interest in ultra-minimally invasive spine surgery (endoscopy) and sacroiliac joint disorders.
He is a pioneer in sacroiliac joint dysfunction, diagnosis, and treatment, and has published on SIJ dysfunction including cooled radiofrequency ablation and a textbook chapter on sacroiliac joint fusion in the Handbook of Spine Surgery.
He works across Norwest Private Hospital, Macquarie University Hospital, and Prince of Wales Private Hospital.
Vincent Fu is one of Sydney's go-to clinicians for complex spinal rehabilitation, post-surgical recovery, and performance-based physiotherapy.
He combines elite-level strength and conditioning with evidence-based physiotherapy and sharp biomechanical reasoning.
Contact
Request a consultation.
Reach out to discuss symptoms, possible evaluation, or next steps in the treatment pathway.
Share where the pain is located, how long it has been present, what treatments have already been tried, and whether the pain is one-sided.